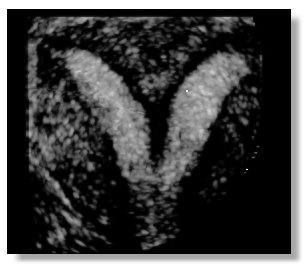
- Bicornute (BU) and Septate Uteri (SU) can look nearly the same on the inside. The interior uterine cavity is divided in two by a kind of wall, which can be made of a vascular or non-vascular material. The wall can sometimes extend through the entire length of the cavity, bisecting it completely. Other times it may only partially divide the cavity.
- Bicornuate and Septate Uteri look very different from the outside. A Septate uterus has a "normal" or domed FUNDUS (the fundus is the top of the uterus, opposite the cervix). A bicornuate uterus has a cleft fundus, following the contour or the interior. A bicornuate uterus looks heart-shaped both inside and out, while a septate uterus has a "normal" shape outside and a heart shape inside
- Bicornuate Uteri are less common and have a relatively good reproductive track record. Issues range from breech positioning to incompetent cervix. I have read that 2nd trimester is the time to be most attentive, when the the fetuses weight is resting on the cervix, not the pelvis.
- Septate Uteri and the most common MA and have one of the worst reproductive outcomes of the MA's, but if threated properly can become statistically normal in pregnancy outcomes. Treatment involves a Lap/Hyst - where a surgeon can physically see the outside of the uterus to ensure it is not cleft, while at the same time, cutting away the septum hysteroscopically. It is an out-patient procedure with about a week recovery time. Doctor's will give you the OK to TTC anywhere from 1-3 months post-op.
- Bicornuate uteri are sometimes, but rarely operated on. This procedure is a major surgery.
- Ultrasound is an exceptionally poor diagnostic tool for determining the difference between a Bicornuate and Septate Uterus.
- MRI can be effective at diagnosing the difference.
- Lap/Hyst is the only SURE way to know what you got.
- A diagnosis of Bicornuate is the "catch-all". If you are told this is what you have via ultrasound, do not proceed with TTC. Make yourself an appointment with a reputable RE and request an MRI followed by a Lap/Hyst.
Please feel free to post comments to me if you are new to the whole MA thing and have questions. I know how scary and confusing it can be.